Case Report
OHVIRA Syndrome - A Case Series on the Spectrum of Presentation
1351
Views & Citations351
Likes & Shares
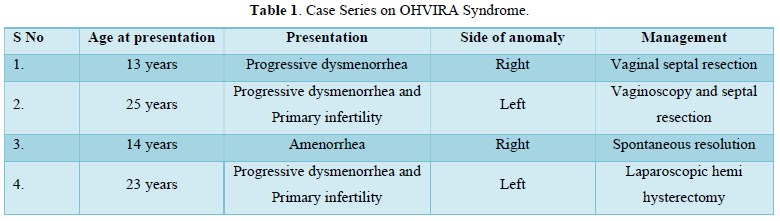
Obstructed hemivagina with ipsilateral renal agenesis (OHVIRA) syndrome also known as Herlyn-Werner-Wunderlich syndrome (HWWS) is one of a Rare Müllerian Anomaly. It is a triad of didelphys uterus, obstructed hemivagina and renal agenesis. Patients usually present after menarche with progressive dysmenorrhea, pelvic masses and rarely late presentations with primary infertility. Such patients are at risk of developing endometriosis, infertility or various obstetric complications. Thus, early recognition and management of such patients is of paramount importance. We hereby report 4 cases of OHVIRA syndrome with a wide spectrum of presentation in relation to menarche and management procedures. First case with early presentation and managed by septal resection. 2nd case with late presentation as infertility and progressive dysmenorrhea and managed by septal resection, conceived later.
The 3rd case is with an early presentation and has a spontaneous resolution. 4th case with late presentation and managed by laparoscopic approach. Through this case series we want to emphasize on the fact that OHVIRA Syndrome needs to be considered in differential diagnosis of patients with progressive dysmenorrhea with menstrual abnormalities.
The 3rd case is with an early presentation and has a spontaneous resolution. 4th case with late presentation and managed by laparoscopic approach. Through this case series we want to emphasize on the fact that OHVIRA Syndrome needs to be considered in differential diagnosis of patients with progressive dysmenorrhea with menstrual abnormalities.
Keywords: OHVIRA syndrome, Progressive dysmenorrhea, Herlyn-Werner-Wunderlich syndrome, Septal resection, Spontaneous resolution
Abbreviations: OHVIRA: Obstructed Hemivagina with Ipsilateral Renal Agenesis; HWWS: Herlyn-Werner-Wunderlich Syndrome; MRI: Magnetic Resonance Imaging
INTRODUCTION
OHVIRA Syndrome is a syndrome of obstructed hemivagina with renal anomaly was first reported in 1922 [1]. In 1980, a triad of didelphys uterus, unilateral obstructed vagina and renal agenesis was named Herlyn-Werner-Wunderlich syndrome (HWWS). The prevalence of OHVIRA syndrome is almost 6.7% but it is up to 25% in women with primary infertility [2]. Rock and Jones classified HWWS into three categories [3]. First category includes the blind hemi-vaginal septum, in such cases there is a uterine horn behind the vaginal septum with no opening and no connection with the contralateral horn. Second category includes blind hemivaginal septum with pinpoint opening. Third category includes hemivaginal septum with cervical fistula, in such cases there is a communication between the two cervices. We hereby report a case series of four cases in which first three cases can be categorized under type II and the fourth case come under type I category. Our case series highlights the varied timing of presentation of cases of OHVIRA syndrome and management options also. Ranging from spontaneous resolution to laparoscopic hemi hysterectomy.
FIRST CASE
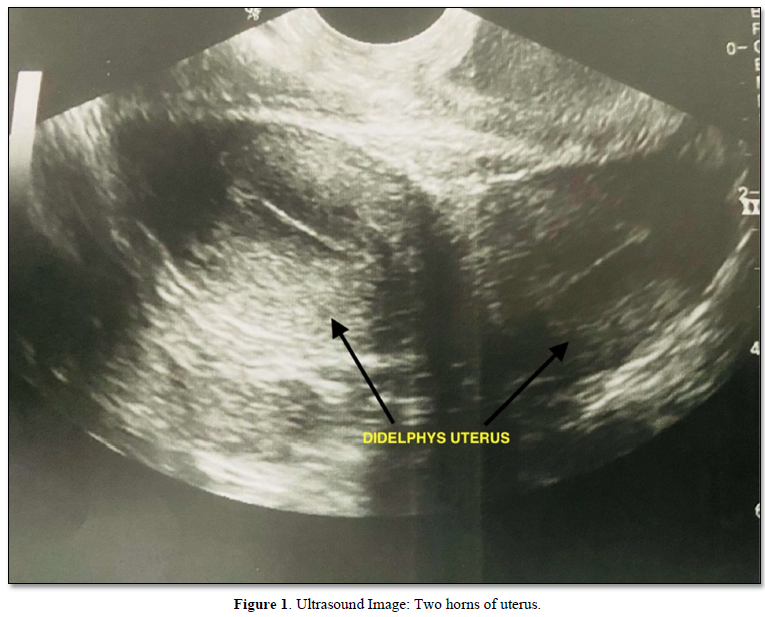
A 13-year- old female presented with complaints of dysmenorrhea and menorrhagia for the past 7 months. She attained menarche 7 months ago and had cycles every 20 days with 7-8-day duration. General examination showed good general condition with no pallor. Abdominal examination was within normal limits. Laboratory tests including complete blood count and thyroid profile were normal. Ultrasound showed a bicornuate uterus with normal echo pattern with a well-defined hypoechoic collection of size 5X5 cm in right sided cervix (Hematocolpos) with normal ovaries. The right kidney was not visualized (Figure 1).
Magnetic resonance imaging (MRI) showed duplicated uterus and cervix with hematosalpinx, Hematometra and hematocolpos on right side suggestive of obstructed right hemivagina. Left hemivagina, uterus and cervix are normal. Both ovaries were normal. The right kidney was not visualized. On the basis of the history and radiological findings the case was diagnosed as OHVIRA or Herlyn-Werner-Wunderlich syndrome. Drainage of Hematometrocolpos with resection of right sided vaginal septum done under general anesthesia. On examination under anesthesia there was a high vaginal septum seen with a bulge of hematocolpos. Left vagina and cervix separately felt from the bulge. Nick given at the bulge of hematocolpos and hematometrocolpos drained and septal tissue resected. Both sides of the cervix visualized and felt. Final diagnosis- uterine didelphys with right sided obstructed hemivagina with right sided hematometrocolpos. Patient was discharged the next day under stable condition.
SECOND CASE
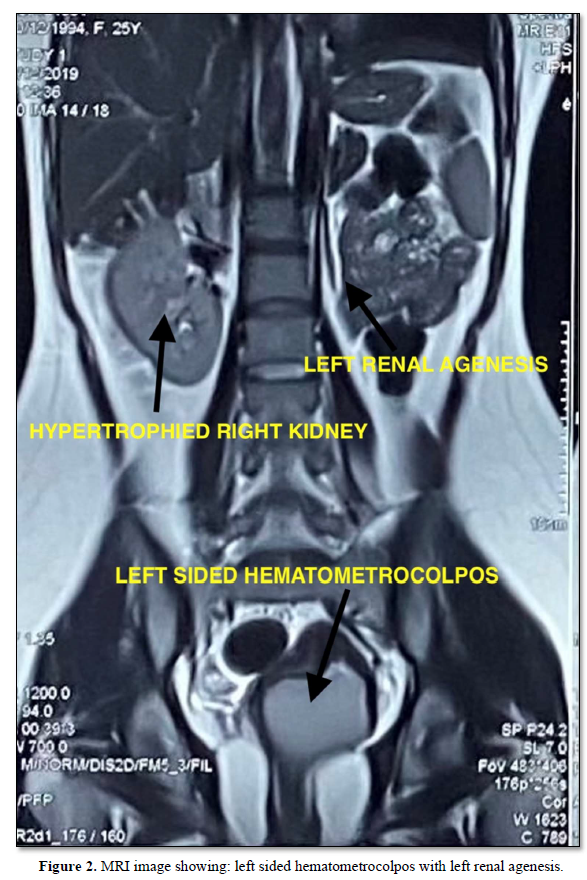
This case is a 25-year-old nulligravida presented with complaints of dull aching pain in the abdomen with worsening dysmenorrhea for the past 10 months. She was married for 3 years. The patient attained menarche at the age of 17 years and had regular menstrual cycles, once every 28 days with 7- to 8- day duration. General physical examination and abdominal examination was within normal limits. Vaginal examination revealed normal right sided cervix which was felt high up and left vaginal wall bulge which was non-tender and cystic inconsistency. Same findings were confirmed by per rectal examination. Ultrasound revealed a bicornuate uterus, left sided endometrioma with hematocolpos. The left kidney was not visualized. Magnetic resonance imaging confirmed the same findings (Figure 2).
Laboratory tests were within normal limits and CA-125 was 14.71. Thus, the patient was diagnosed with OHVIRA Syndrome. Under general anesthesia vaginoscopy was performed and vaginal septum resection was done. During vaginoscopy a bulge was seen on the left lateral wall which was extending up to introitus. A normal right sided cervix was seen. Incision was given over the bulge using a resectoscope on the upper end of the bulge. After the drainage of hematocolpos, the left sided pinpoint hole cervix was identified. Vaginal septum was excised and reefed. On follow up patient had dysmenorrhea only. She conceived twice after ovulation induction therapy. First one was a missed abortion in first trimester. In her second conception, currently her period of gestation is around 20 weeks and uncomplicated till date. Her antenatal ultrasounds showed left sided 3X3 cm endometrioma and live intrauterine pregnancy in the right horn. Her aneuploidy screening is within normal limits. Anomaly scan was normal with cervical length of 3.2 cm.
THIRD CASE
A 14-year-old female presented with a complaint of pain abdomen with amenorrhea for 5 months. The patient attained menarche at the age of 13 years and had regular menstrual cycles for 4 months. Patient had flow for 3- to 4-days duration with no dysmenorrhea.
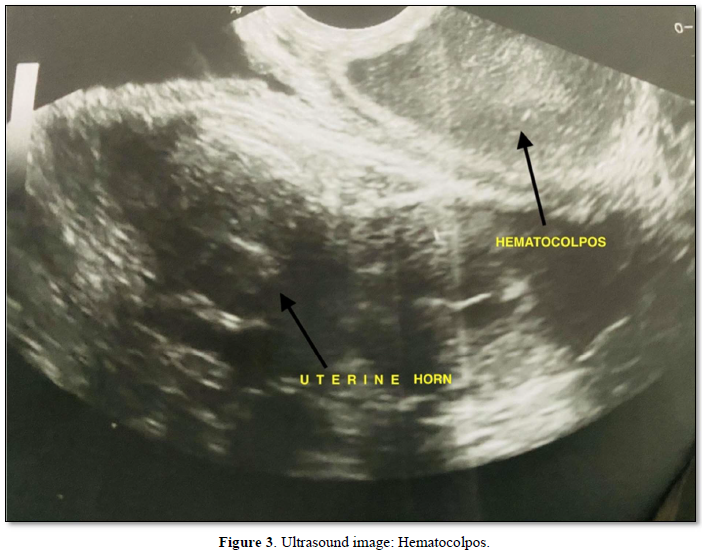
After that the patient had amenorrhea for 5 months accompanied by pain in the abdomen. Her general physical and local examination was unremarkable. She was investigated for amenorrhea. Her laboratory investigations and hormonal profile was within normal limits. Ultrasound showed a bicornuate uterus with hematometra in the right horn and left horn endometrial thickness of 11mm. 6X9cm hematocolpos (Figure 3) seen behind the urinary bladder. The right kidney is not visualized with the normal left kidney.
While the patient was being evaluated for amenorrhea, she had spontaneous bleeding per vaginum for which she presented in our outpatient department. Abdominal ultrasound was repeated to show normal bilateral horns of the uterus with resolved hematometra and hematocolpos.
FOURTH CASE
This is a case of a 23-year-old nulliparous female married for 2 years. She presented with complaints of primary infertility with progressive dysmenorrhea. No other significant past or family history was elucidated. She attained menarche at the age of 14 years with regular cycles and normal flow till date. For the last 6-7 months the patient had progressive dysmenorrhea. She is cohabitating with her husband and has been trying to conceive since her marriage. Her general physical and abdominal examination was within normal limits. Local examination showed a right sided cervix which was pushed laterally and downwards. There was left sided forniceal fullness seen and same confirmed on bimanual examination. Exact size of the uterus could not be appreciated. Husband semen analysis was within normal limits. Ultrasound showed didelphys uterus with 5x4 cm collection in vaginal canal with an impression of transverse vaginal septum. Ultrasound also showed an absent left kidney.
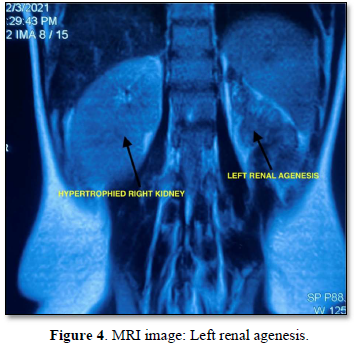
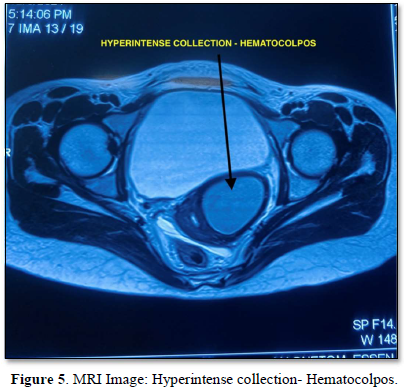
MRI also showed two separate uterine cavities with divergent apices with two cervices and single vagina, findings suggestive of didelphys uterus. There was left sided renal agenesis and hypertrophic right sided kidney (Figure 4). Hyperintense loculated collection seen in lower left cervical region suggestive of hematocolpos (Figure 5). Vaginal septum is seen on the same side. Right sided Mullerian structures were within normal limits.
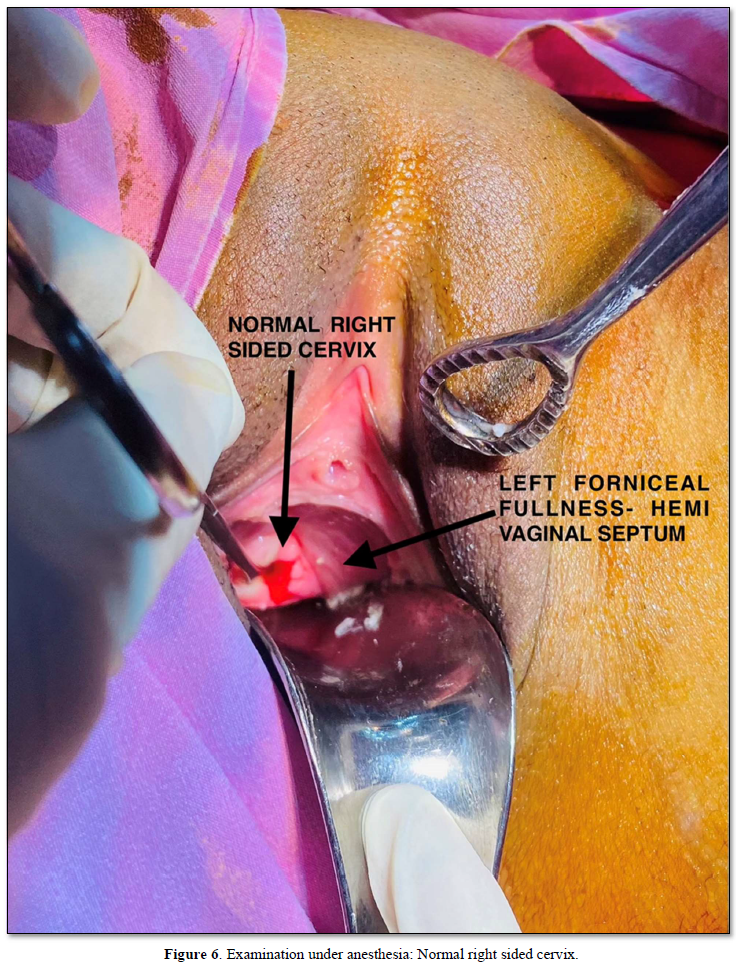
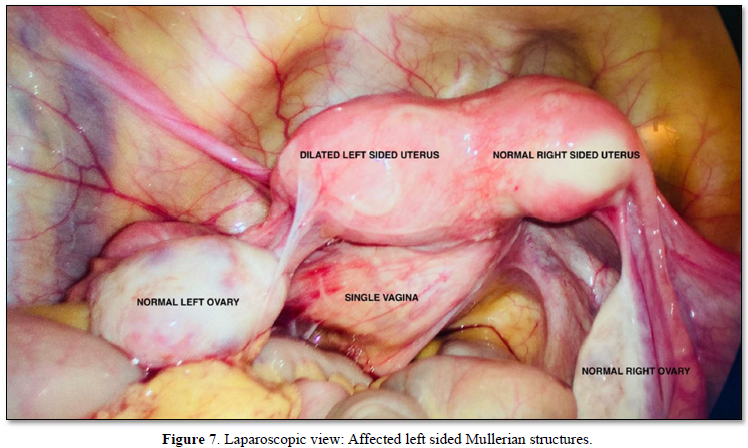
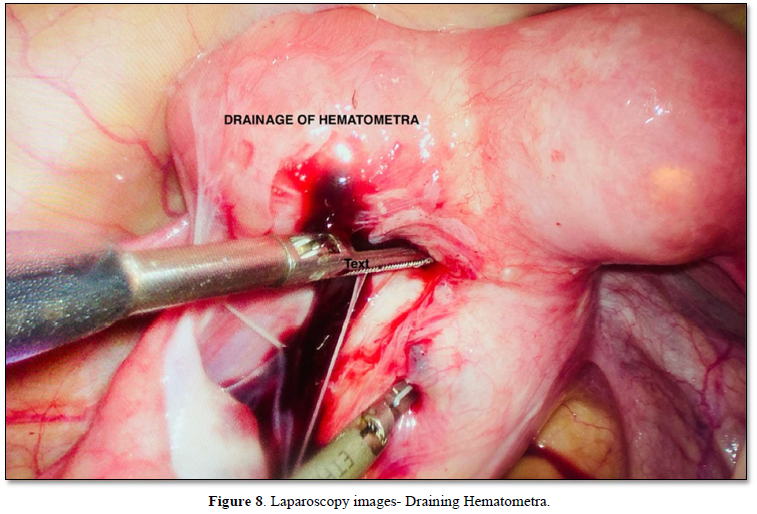
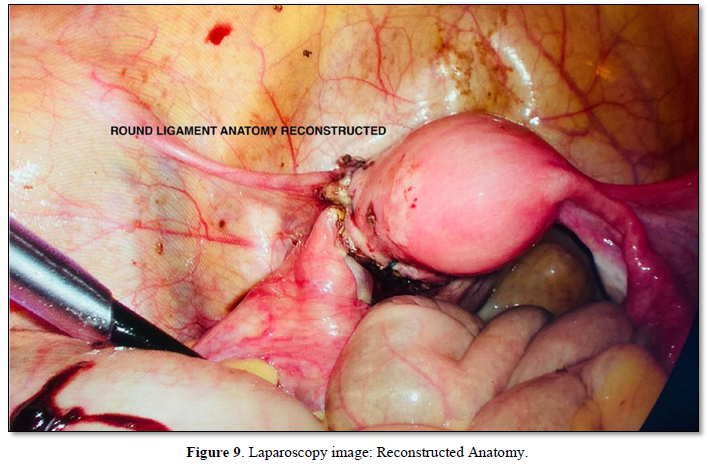
Thus, based on clinical and radiological findings the patient was taken for laparoscopy and examination under anesthesia. Under anesthesia the right sided cervix normally seen with left sided forniceal fullness felt (Figure 6). Needle aspiration tried through the vaginal septum but no aspirate retrieved. On laparoscopy two separate uterus seen (Figure 7) with endometriotic spots seen on uterus and fallopian tube of left side. Hemi hysterectomy done chocolate colored fluid seen coming out (Figure 8). Anatomy of the round ligament and uterus reconstructed thereafter (Figure 9). Her postoperative period remained uneventful and the patient was discharged after two days. All the above cases are summarized in Table 1.
DISCUSSION
OHVIRA syndrome is one of the rare Mullerian duct anomalies. It compasses obstructed hemivagina with uterovaginal duplication accompanied by renal agenesis of the ipsilateral side. Precise etiology of OHVIRA Syndrome is still unknown. It has been hypothesized as an aberrant development of mesonephric and paramesonephric ducts. The mesonephric ducts, also known as wolffian ducts are inductors for the development of paramesonephric ducts. Therefore, abnormalities in the development of mesonephric ducts lead to renal abnormalities. These are often accompanied by the abnormal development of the uterus and vagina. OHVIRA Syndrome encompasses a wide spectrum of presentations ranging from menstrual abnormalities, dysmenorrhea, pelvic or paravaginal masses to acute abdominal pain and acute urinary retention [4]. All these presentations occur due to outflow obstruction related complications. The latter include hematocolpos, hematometra, retrograde bleeding, endometriosis all these leading to formation of pelvic adhesions and infertility. Two out of four cases had an early presentation near menarche as commonly reported. Many cases may have delayed presentations attributed to absorption of accumulated blood in between the menses, as seen in our second case. Delayed presentation is reported up to 41 years of age [5]. Successful pregnancy outcomes are also reported in literature with cases of spontaneous conception with term deliveries [6]. Our second case had an ovulation induction conception with mid trimester pregnancy without any complication till date.
It is a rare type of Mullerian duct anomaly associated with an increased risk of infertility, endometriosis and pelvic adhesions formation. Thus, this entity needs to be identified and diagnosed at the earliest to prevent consequences in future. Due to a rare entity and presence of regular menses from the unobstructed hemivagina, diagnosis of HWWS is often delayed leading to undiagnosed chronic HWWS. It is very difficult to diagnose HWWS due to non-specific presentations. Multimodal approach is usually required for such a diagnosis which integrates clinical history, examination findings and investigations. Various investigations may help which include ultrasound (USG), Magnetic resonance imaging (MRI) and laparoscopy or hysteroscopy for direct visualization. We used the above approach in our cases for diagnosis, which was later confirmed intraoperatively also.
Ideal treatment option for HWWS is still a debatable point as there is no standard clinical course of this pathology and each patient needs to be individualized. Our third case showed the possibility of spontaneous resolution of such cases. OHVIRA Syndrome is definitely managed with the resection of vaginal septum and drainage of hematometrocolpos. But in literature there are cases reported with spontaneous resolution or managed with hemi hysterectomy [7], as seen in our patients. Our fourth case can be classified as under category I of rock jones classification [3], with no opening behind the vaginal septum, as confirmed by needle aspiration through the vaginal septum and thus managed by hemi hysterectomy.
CONCLUSION
There are enormously variable presentations and effects of different congenital anomalies on the female genitourinary tract. To understand such complex pathologies the basic knowledge of the development of the embryological system is required. Through this case series we provided detailed descriptions of various important scenarios related to heterogeneous presentation, management options with possibility of spontaneous resolution. We also highlighted the possibility of pregnancy in patients with OHVIRA syndrome. Thus, OHVIRA syndrome must be kept in the list of differential diagnosis in young females presenting with pelvic masses or progressive dysmenorrhea or renal tract abnormalities. Early identification and immediate surgical intervention help in preventing future complications.
- Purslow CE (1922) A case of unilateral hematocolpos, hematometra and hematosalpinx. J Obstet Gynaecol Br Emp 29: 643.
- Chan YY, Jayaprakasan K, Zamora J, Thornton JG, Raine-Fenning N, et al. (2011) The prevalence of congenital uterine anomalies in unselected and high-risk populations: A systematic review. Hum Reprod Update 17: 761-771.
- Rock JA, Jones HWJ (1980) The double uterus associated with an obstructed hemivagina and ipsilateral renal agenesis. Am J Obstet Gynecol 138: 339-342.
- Mandava A, Prabhakar RR, Smitha S (2012) OHVIRA syndrome (obstructed hemivagina and ipsilateral renal anomaly) with uterus didelphys, an unusual presentation. J Pediatr Adolesc Gynecol 25: 23-25.
- Kriplani A, Dalal V, Kachhawa G, Mahey R, Yadav V, et al. (2019) Minimally Invasive Endoscopic Approach for Management of OHVIRA Syndrome. J Obstet Gynaecol India 69: 350-355.
- Albulescu DM, Ceauşescu AE, Sas LM, Comănescu MC, Constantin C, et al. (2018) The Herlyn-Werner-Wunderlich triad (OHVIRA syndrome) with good pregnancy outcome - two cases and literature review. Rom J Morphol Embryol 59: 1253-1262.
- Yoder IC, Pfister RC (1976) Unilateral hematocolpos and ipsilateral renal agenesis: Report of two cases and review of the literature. AJR Am J Roentgenol 127: 303-308.
-
 Table 1
Table 1










QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Carcinogenesis and Mutagenesis Research (ISSN: 2643-0541)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Pathology and Toxicology Research
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Advance Research on Alzheimers and Parkinsons Disease


